Medicare is sustainable,
for-profit care is not.
BRIEFING NOTE
Canadian Health Coalition
www.medicare.ca
Ottawa, May 14, 2004
ISSUE
Canadians are being told that Medicare is not
sustainable and that spending must be shifted from public to private budgets and delivery.
BACKGROUND
Prime
Minister Martin has called for a First Ministers’ Conference (FMC) this summer to
adopt a 10-year Medicare ‘sustainability’ plan.
The premise of the plan appears to be that our health care system is
unaffordable and that the provinces need to make major changes. Claims are also made that
cost increases are crowding out other government priorities. These claims are
unsustainable, based on the data.
According to a Finance Department
study, health care will remain affordable over the next 40 years. Share of total health
care expenses for Canada will likely remain less than 10 per cent of the Canadian economy.
Current health care spending is 9.8 per cent of GDP (Jackson
and McDermott, 2004).
Public health care
expenditures are not exceeding public resources. The parts of health care expenditures
that are out of control are those not covered by the Canada
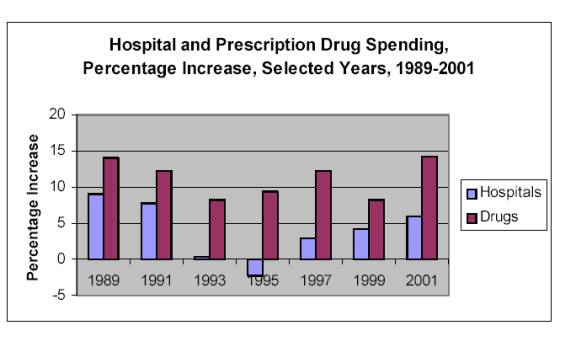
Health Act; especially drugs. Drug costs have tripled as a share of national income in
20 years. Medicare spending (hospitals and physicians) takes up the same share of national
income as 20 years ago.
Claims that Medicare is
financially unsustainable are part of a broader campaign to advance the priorities of tax
cuts, smaller governments and the expansion of investor-owned health care delivery.
This agenda is a perversion
of the core Canadian value of equal access to health care for all, financed on
income-based taxation. The vast majority of Canadians believe safeguarding equal and
timely access to public health care is more important than tax cuts.
In the words of the Romanow
Report: Canadians have been clear that they still
strongly support the core values on which our health care system is premised –
equity, fairness and solidarity…They want and they expect their governments to work
together to ensure that the policies and programs that define medicare remain true to
these values.
CONSIDERATIONS
1. Financial pressures are from drug costs, not
Medicare
In 2002, hospital and physician services
accounted for 4.3% of national income, down from 4.5% in 1971. The share of national
income devoted to public health insurance programs has been remarkably stable.
Expenditures on prescription drugs, on the other hand, which are outside of Medicare, have
been growing rapidly, more than tripling their share of national income since 1980. The
drug industry claims that this increase has reduced hospital costs. This claim
“cannot withstand any serious empirical scrutiny” (Evans, 2003).
|
 |
|
Universal, comprehensive
coverage is not more expensive than the fragmented mix of public and private insurance
coverage and out-of-pocket payment that existed before Medicare. Consolidation of
expenditures in the hands of a single payer made it possible to control costs and expand
access. If services are not affordable for a society on a universal basis through a single
payer, not-for-profit system, they are not affordable in an American-style system of
for-profit delivery.
Why would those who say the Canadian health-care
system is in a fiscal crisis and headed for collapse focus on the public insurance programs, hospital and physician
expenditures? Why would any rational person, concerned about rising costs, advocate
transferring costs from government budgets back onto patients, either directly or through
increased private insurance contributions? Based on all available evidence, such a shift
would almost certainly lead to more rapid
escalation of health spending.
2.
The real motives: narrow self-interest
The
data shows Medicare is sustainable. So what are the real motives behind the talk of
Medicare’s unsustainability? A powerful elite, pursing a narrow self-interest, wants
access to the best health care money can buy without having to pay the taxes needed to
provide equal access for all Canadians. Some of those elite also stand to benefit
financially from selling private health care services.
Universal, tax-financed health care requires
higher-income people to contribute more to support the system, without offering them
preferred access or a higher standard of service. Private financing reduces the burden on
the wealthy because they are healthier. Private payments limit access by people with lower
incomes and thereby open better access for those willing and able to pay.
Moving away from fully
tax-financed public insurance would let the wealthy pay
less (in charges, private premiums and taxes) and get more (in volume, quality, and/or
timeliness). Those with lower incomes would pay more and get less. This conflict in
economic interest is real, unavoidable, and present in all societies. This explains why
the “public/private” debate never goes away. (Evans, 2003)
Policy proposals for structural “reform” are
in reality, attempts to redistribute burdens and benefits. Private health care is not only
a perversion of Canadian Medicare values. It is also less efficient, more expensive and
diverts care from those with greatest needs to those with greatest resources. Private
health care is fraught with fraud and higher death rates. But a small elite still come out
ahead.
Claims that Canada’s
Medicare is economically or fiscally unsustainable are part of a broader campaign to
advance the priorities of the few at the expense of the many.
3. For-profit health care
is not sustainable
Sustainability is also a code word for
"privatization" and "for-profit care."
Increased privatization depends upon an argument that public healthcare is
unsustainable. Once we accept that premise,
then it is a simple matter to turn health services over to for-profit corporations. Recent
evidence has shown that private for-profit ownership of hospitals, in comparison with
private not-for-profit ownership, results in a higher risk of death for patients (Deveraux, 2002).
Federal, provincial and
local governments contribute approximately $85 billion in taxpayers’ money to our
health care system. Twenty billion of that is
federal money transferred to the provinces under the new Canada Health Transfer. This is money that profit - making corporations
would dearly like to get their hands on.
Privatization of existing
publicly delivered health services are their preference.
Private surgical clinics and hospitals providing joint replacement or
eye surgeries are prime targets. So are diagnostic clinics for CT, MRI and PET scans, and
long term care and home care services. Corporations
prefer single payer arrangements because they constitute the contracting out of public
services with a guaranteed government revenue stream to the for-profit service provider. In fact, in some cases such as long term
care and home care they would even prefer increased public spending for private for-profit
care – so much for their sustainability concern.
Much has been made of
"eliminating waiting lists" and "guaranteed waiting times." It is
essential that we make reforms to Medicare so that accessibility to health care services
is timely. However, the reform presented by
corporate health care providers is simply to contract services out to investor owned
health care providers, padding their pockets with public money, doing little to reduce
waiting times, and doing nothing to improve efficiencies and sustainability. And in the process two – tier health care
will be established where those who can afford to pay privately and jump the queue, will.
The real message is that private,
for-profit health care is not sustainable. Waiting
lists are reduced only for those who can afford to pay. Studies have shown that public
waiting lists for cataract surgeries are longer when there is a parallel for-profit system
in operation. According to Alberta Health (http://www.health.gov.ab.ca/system/funding/performance/Cataract.pdf)
average wait times for cataract eye surgery in Calgary, where 100% of surgeries are done
privately, almost three times longer than Edmonton, which is 80% public. Costs will not
decrease. For-profit corporations will pursue
more public money and will sacrifice care for profits.
Public private partnerships (P3s), often pitched as the
panacea for sustainability problems for hospitals, actually result in fewer hospital beds
in the community, reductions in health care personnel and a decrease in the quality of
care. P3s do not contribute to
sustainability for health care as they cost more than public infrastructure financed with
public dollars. Public expenditures on health care are not diminished. See Auerbach et
al. “Funding Hospital Infrastructure: Why P3s Don’t Work and What
Will”. http://www.policyalternatives.ca/publications/p3-hospitals-summary.html
4. Federal health care
spending at historic lows
Federal
support has languished for the national program Canadians value most. Under Finance
Minister and now Prime Minister, Paul Martin, federal spending on all programs as a
percentage of the gross domestic product (GDP) has fallen to 1949 levels. Martin has
ushered in a ‘Permanent Revolution in Government’ (Yalnizyan, 2004a) of smaller government and bigger
markets.
Between 1995/96 and 1997/98, Finance Minister Martin
cut federal cash transfers by $5 billion, or nearly 20%, leaving a substantial hole in
provincial and territorial budgets. The federal strategy was very successful in shifting
the deficit onto the backs of the provinces and territories. At the same time, the
Government of Canada has been recording major surpluses since 1997/98 and seems likely to
do so for the indefinite future. Rather than restoring the cash grants to their pre-Canada
Health & Social Transfer rate, Finance Minister Martin chose to cut federal income tax
rates.
Chart 2: Federal real per capita health support is at
historic lows
Source:
Provincial data CIHI, NHEX Table B4.7, 2001; federal data calculated from Finance
Department data), updated to reflect the September 2000 agreement, in Yalnizyan, 2004b.
5. Public health care,
other program spending, and tax cuts
From 1995/96 to 2001/02,
health spending by all provincial and territorial governments in Canada rose from 34.8% of
total program spending to 41.1%. This trend is used to make the claim that escalating
health care costs in the public sector are increasingly crowding out other important forms
of public expenditure – clearly an unsustainable situation. Allegedly, this problem
can be addressed only by transferring costs from public to private budgets.
Both the total spending by
provincial governments and spending on Medicare programs alone, took up roughly the same
share in 2001/02 as in 1995/95, a share little different from twenty years earlier. So why
are we now being told that health care spending is “crowding out” education and
other social programs?
Chart 3 Provincial
Government Expenditure as percent 0f GDP - 1980/81 to 2002/03
Source: Evans, December 2003 (data updated in 2004).
In light of this reality, it
follows that provinces must have been cutting back on their non-health spending, and
indeed they were. The myth of health care “crowding out” other program spending
implies that health spending was rising as a share of provincial revenues as well as of
program expenditures. This is not so. Medicare spending now takes up roughly the same
share of provincial revenue as it did twenty years ago.
The
truth is that right-wing governments in several large provinces chose tax cuts and deeper
cuts to non-health programs. Further cuts to
health spending were more politically difficult. In this sense, one could say health care
“crowded out” other programs. But
it would be false to claim that an unsustainably expensive public health care system has
been the source of the pressure on other programs. (Evans, 2003)
These choices were not due
to fiscal necessity from poor economic performance. Rather, it was a political decision to
take advantage of an improved economy to cut taxes rather than maintain spending on public
programs.
6. Are
human rights and compassion sustainable? Values in conflict
What
is it that needs to be sustained? Canadians have made it clear that they care about equal
access to health care for all Canadians. Canadians rated equal access to health care for
all as the area of greatest concern in health care in polling from 1995 to 2003.
The value of equal access is not shared by everyone in society. For example, Michael Kirby, a director of
Extendicare Inc., a for-profit nursing home chain, authored a Senate report which asks:
“Is it fair to deny people who can afford to buy health services the right to buy
those services?” (Senate Health Committee Report, Volume 4, p. xv). Senator Kirby
feels so strongly about his libertarian values that he intervened with nine other senators
in a Supreme Court case to argue that Canada’s public health insurance and hospital
legislation should be struck down as unconstitutional. http://www.healthcoalition.ca/chaoulli.html
Only
18 per cent of Canadians would allow for privatized health care where money can buy you
better care or quicker access.
The
debate over the sustainability of Medicare is primarily about ethics and values, not
economics and finances. Some politicians today want us to believe there isn’t enough
public money to provide health care for everyone, but somehow, privatizing health care
services and driving up costs`, will make it more affordable for the public. Beware of
this deception. There is only one taxpayer.
In
the words of the recent Finance Department study: “Given the wide range of spending
options that are fiscally feasible, discussions of sustainability ultimately become a
question of public choice.” (Jackson and
McDermott, 2004).
‘Medicare
is as sustainable as we want it to be’. (Romanow).
Citizens
in a democracy are the ones to determine what share of our collective wealth ought to be
spent on Medicare.
RECOMMENDATIONS
To ensure that Medicare is
sustainable, the Canadian Health Coalition recommends the following:
1.
Restore federal cash transfers to at least
25% of total health care costs - which includes the full continuum of care - from
prevention and promotion through to home and community care, acute care, palliative and
long-term term care. Establish a transfer escalator to ensure federal share is maintained
over time. Attach strings and conditions so new money goes to public health care not
provincial tax cuts.
2. Direct
public funds to care not profits. Tax dollars are
for giving care not taking profits. To prevent commercial waste of tax dollars, loss of
public accountability and threats to patient safety, a moratorium must be placed on any
initiatives to privatize the delivery of health care services and a prohibition on all
public private ‘partnerships’ in health care. Health care belongs in the public
sector not in the hands of private investors.
3. Use the new
money to buy change. Establish national standards
for home and long-term care, including not-for-profit delivery. Coordinate a national
pharmaceutical strategy. To ensure safety, access and affordability, the strategy must
include cost controls, a public drug information system, improved access to generic
alternatives, enforcing the ban on
direct-to-consumer drug advertising, and effective monitoring of adverse drug reactions.
4. Reduce waiting times with
stable funding to ensure public capacity for the full continuum of health services
including diagnostics, home and long-term care, 24/7 access to care, human resource
planning and publicly financed capital investments. Waiting times are about planning for
care. This requires stable funding and a plan. Wait time guarantees are counter-productive
and result in perverse incentives that encourage two-tier for-profit care.
5. Address the social determinants of health, including affordable housing, for all Canadians and especially
for First Nations, Inuit, and M�tis peoples. Improve access to all levels of health care
services and recruit new Aboriginal health care providers.
6. Enforce the Canada Health
Act’s five criteria (public administration,
comprehensiveness, universality, portability, accessibility) and two conditions
prohibiting extra-billing and user fees. Correct the deficiencies in monitoring, reporting
and enforcing compliance.
7. Health Promotion and disease prevention requires that the federal government uphold the duty of care in
the Food & Drugs Act. Terminate proposal for new Canada Health Protection Act.
Preventable damages from adverse drug reactions, food-borne pathogens, and hazardous
medical devices - threaten the health of Canadians and the sustainability of Canada’s
health care system.
8.
Protect the health care system from trade
agreements by negotiating a general
exclusion in trade agreements for health services and health insurance.
REFERENCES
Lewis Auerbach, Arthur
Donner, Douglas D. Peters, Monica Townson, and Armine Yalnizyan, Funding Hospital Infrastructure: Why P3s Don't Work,
and What Will, Canadian Centre for Policy Alternatives, November 2003. http://www.policyalternatives.ca/publications/p3-hospitals-summary.html
P.J. Deveraux,
“A Systematic review and meta-analysis of studies comparing mortality rates of
private for-profit and private not-for-profit hospitals”, Canadian Medical Association Journal, May 28,
2002 http://www.healthcoalition.ca/CMAJ.pdf
Robert
G. Evans, Political Wolves and Economic Sheep: The
Sustainability of Public Health Insurance in Canada, Centre for Health Services and
Policy Research, UBC, December 2003 http://www.chspr.ubc.ca//chspr/pdf/chspr03-16W.pdf
Harriet Jackson and Alison
McDermott, Health Care Spending: Prospect and
Retrospect, Analytical Note, Economic and Fiscal Policy Branch, Department of Finance,
January 2004. www.healthcoalition.ca/finance-note.pdf
Armine Yalnizyan, Paul Martin’s Permanent Revolution,
Alternative Federal Budget 2004 Technical Papers #3, Canadian Centre for Policy
Alternatives, 2004. http://www.policyalternatives.ca/
Armine Yalnizyan, “The
Health Care Budget: Did it resolve the ‘Crisis’?”, in Charles Beach and
Thomas Wilson, eds., The 2003 Federal Budget:
Conflicting Tensions, Kingston: John Deutsch Institute, 2004b, pp. 231-262.
Public money is for patients, not profits.
www.medicare.ca
| Finance Says Medicare is Sustainable Globe
and Mail, Apr. 15, 2004 |
By HEATHER SCOFFIELD |
|
|
|
Ottawa — Health care will remain affordable over the next 40
years as long as the economy and private spending continue to grow at a moderate pace,
says a new internal Finance Department study obtained by The Globe and Mail.
The analysis from the department's fiscal-policy division was
written in January and discounts predominant theories that rising health-care costs will
bankrupt federal and provincial governments unless serious reforms are undertaken.
The study argues that although health-care costs will continue to
rise, historical spending patterns show that governments will have enough money to pay
their share of the bill for decades to come.
The aging population alone will not drive up costs
astronomically, as many fear, said Alison McDermott, who wrote the report with fellow
economist Harriet Jackson.
"As the country gets richer, it will be able to afford more
for health care as well," Ms. McDermott said in an interview yesterday.
"The projections show sizable increases in total health-care
spending as a share of GDP over the next 40 years," says the study, which will be
expanded upon and turned into a public working paper. "However, scenarios believed to
be most plausible appear manageable from a fiscal standpoint."
Their conclusion challenges assumptions that dominate thinking on
health care across the political spectrum. The federal government is seized with the issue
of how to make funding sustainable on a long-term basis, assuming that costs are rising
too quickly for Ottawa and the provinces to carry on.
Last week, Prime Minister Paul Martin approved the hiring of
economist Paul Boothe, director of the University of Alberta's Institute for Public
Economics, as a top-ranking official at the Department of Finance. Mr. Boothe is known for
his radical ideas on health-care funding, and has proposed that patients be forced to pay
for some of their costs, based on income.
Mr. Martin has made it clear that reforming health care is his
priority and that he wants to have a 10-year plan to make sure Canada can pay for publicly
funded health care.
The premise of the plan is that health care in Canada is in
serious trouble and that the provinces need to make major reforms for the federal
government even to contemplate increasing funding.
But the internal Finance Department document could undermine that
premise. The authors say governments' share of total health-care expenses for the country
will likely remain less than 10 per cent of the size of the Canadian economy. Right now,
public and private health care in Canada together amount to 9.8 per cent of gross domestic
product. The study concludes that increasing expenses can be shouldered by both the public
and the private sector.
"The total government sector looks to be quite
sustainable," Ms. McDermott said. |
|
|